60 year old female with pain abdomen and decreased urine output
Date 24.4.23
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment
A 60 year old female, housewife, a resident of mungole, came to casualty with chief complaints of pain abdomen since 4 days and decreased urine output since 4 days.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 4 days ago, then she developed pain in the abdomen, left lumbar region, insidious in onset and gradually progressive, radiating to lower abdomen and back. It was of dragging type and diffuse. There are no aggravating or relieving factors. There is pedal edema associated with it, non pitting type. No facial puffiness, loin pain. Patient also had decreased urine output, hesitancy, since four days which was insidious in onset. The urine was pale yellow and clear. It was associated with burning micturition. No history of nocturia, dysuria, urgency, frequency, urethral discharge, pyuria. There is no history of fever, diarrhoea, constipation.
PAST HISTORY:
There are no similar complaints seen in the past. Patient is a known case of Diabetes Mellitus since 7 years and is on OHA and soluble insulin. Patient is also a known case of Hypertension since 7 years and is on Telmisartan 40mg. Patient is a not a known case of TB, CVD, epilepsy, blood transfusions and thyroid disorders.
FAMILY HISTORY:
No similar complaints seen in the family.
PERSONAL HISTORY:
Diet is mixed, appetite is normal, sleep is adequate, constipation and decreased urine output is present. She takes betel leaf. No smoking or alcohol. No known allergies.
GENERAL EXAMINATION:
Patient is conscious, coherent and cooperative. Well oriented to time place and person. Moderately built and moderately nourished. Pedal edema is present, non pitting type. No signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy.
Temp: afebrile PR: 89bpm RR: 22cpm BP: 130/90mmHg SpO2: 99%
SYSTEMIC EXAMINATION:
Per abdomen:
On Inspection, shape of abdomen is obese, flank fullness is present. Striae vascularis is present, no linea nigra present. No sinuses, hernial orifices, dilated veins, visible pulsations. Umbilicus is centrally placed, inverted. No pigmentation.
On Palpation, all inspectory findings are confirmed. No local rise of tenderness. Tenderness present in the left lumbar region. Liver and spleen are not palpable.
On Percussion, fluid thrill is present. No shifting dullness.
On Auscultation, bowel sounds are heard


CVS: S1S2 heard; no murmurs heard
Resp: NVBS + BAE +
CNS: NAD +

PROVISIONAL DIAGNOSIS:
Renal stones..? AKI..? Pancreatitis..?
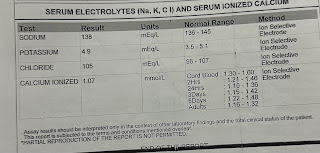
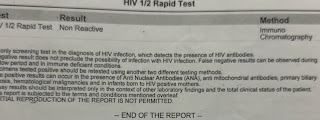
INVESTIGATIONS:

















TREATMENT:
1. TAB.TAXIM 200mg PO/BD
2. TAB.CINOD 10mg PO/BD
3. INJ.LASIX 40mg IV/BD
4. TAB.PAN 40mg PO/OD
5. INJ BUSCOPAN IV/SOS
6. TAB PCM 500mg PO/SOS
7. SYP CITRALKA 15ml in 1/2 glass of water PO/BD
8. TAB DROTIN DS PO/BD
9. TAB ZOFER 4mg PO/BD


Comments
Post a Comment